
*The RITA-T Team has updated the administration of item I: Mirror: Self-Recognition. Please check back on the course site or our website for updates as we continue to develop this. Updates to the training course and RITA-T material are made accordingly. *
The RITA-T is an interactive and observational Level 2 screening measure that has been validated extensively on young children (toddlers) ages 18-36 months. The RITA-T can be administered on young children identified at risk for ASD: either by a high score on a level 1 screener, or because of concerns brought up by their caregivers or providers.
Examples of a Level 1 or universal screener include the MCHAT-R (Modified Checklist for Autism in Toddlers - Revised) that may or may not have been administered before the RITA-T. You can go here to learn more about the MCHAT-R.
Examples of young children at risk include: siblings of a child already diagnosed with ASD, children born with higher risks for neurodevelopmental disorders such as: prematurely born children, children already identified with other delays and in Early Intervention Programs, or those with genetic disorders known to be associated with ASD (such as Trisomy 21).
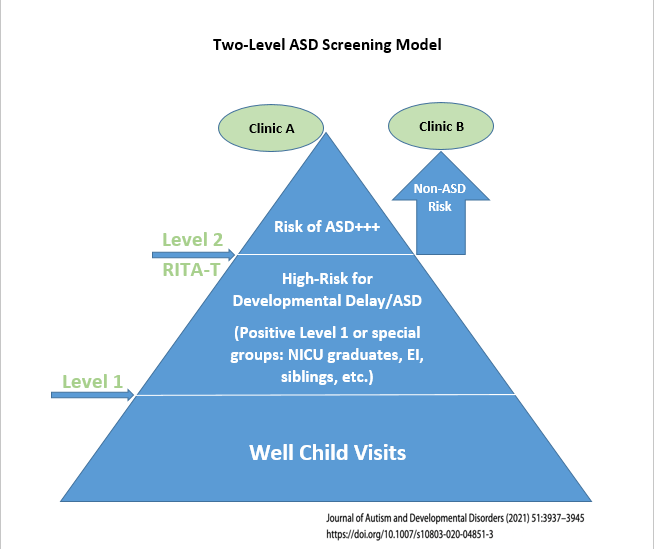
A Level 2 screener can be administered to this group of high-risk children to differentiate between ASD and other delays (See figure below that depicts a Two-Level ASD Screening Model). This will result in identifying the children who are really at risk for ASD and thus refer them in a faster way for more appropriate ASD evaluations. An interactive Level 2 test is preferred in this age group (18 months-36 months) as it allows the direct observation of the early signs we are looking for rather than relying on history, as they may be hard to recognize.
RITA-T Test Constructs Evaluation
The RITA-T includes nine semi-structured play-based activities that examine constructs that have been described to be delayed in children with ASD. Each play-based activity allows the observation of the child’s response. Signs that are evaluated are: Joint Attention (JA), Human Agency (HA) that is the precursor for the Theory of Mind, Social Awareness (SA), Communication, Self-Awareness, and there is an element of visual reception assessment.
Three items are related to the developmental level of the child and coded C for Cognition. Each activity is coded and scored depending on the child’s response: the lower the score, the more typical the response. A total score is calculated by adding the scores of the 9 individual activities.
A RITA-T manual and a RITA-T scoring sheet have been developed and validated. The RITA-T manual describes the administration and scoring of each one of the items. The manual and the RITA-T scoring sheet can be obtained and downloaded from the RITA-T online course package.
RITA-T Details
- Validated and Reliable in 18-36 month olds
- Easy to train on and learn
- Can be administered in approximately 20 minutes
- The training for reliable administration and scoring of the RITA-T is easily accomplished in about 3 hours of targeted training within a small group of clinicians
- The RITA-T differentiates extremely well between toddlers with ASD and toddlers with Developmental Delay (DD)/Non-ASD at cut off scores that have been consistent across different settings such as:
- Scores >16 are highly associated with ASD and a PPV of 98-99%
- Scores 12-16 are considered medium risk range but still have a PPV of 95-98% for ASD
- Scores below 12 are considered low risk for ASD
- As for any interactive measure, clinical judgement still prevails
- The RITA-T correlates well with established diagnostic measures of ASD such as DSM-5 ASD criteria; the Autism Diagnostic Observation Schedule – second edition (ADOS-2) and modules Toddler and 1; the Childhood Autism Rating Scale-2 ST (CARS-2ST).
- Early Childhood providers in different specialties have trained on the RITA-T: primary care providers (MD, NP, PA), psychologists, developmental behavioral pediatricians, neurologists, child psychiatrists, early intervention and therapists such as developmental specialists, speech therapists, occupational therapists, social workers
- Fits well into a busy practice flow
- The RITA-T does not rely on language so it can be used in non-English speaking children.
- Scoring sheets and Manual have been translated and validated to: Turkish, French, Chinese, and Arabic
- They have been translated to Spanish and Portuguese
- Tele-RITA-T and preliminary data also available in the course